
As the Patient Driven Groupings Model (PDGM) looms on the horizon, home health officials will need to rethink diagnosis coding and billing strategies to ensure their business maintains financial stability. New rules covering low-utilization payment adjustments (LUPAs) and coding multiple secondary diagnoses are capturing the attention of home health agencies.
Reimbursement rates overall are declining as well. In late October, the Centers for Medicare and Medicaid Services (CMS) announced that the final behavior change adjustment for PDGM 30-day payment rates would be a 4.36% reduction instead of the proposed 8.01% decline. CMS said the change in the rate was made in consideration of comments from industry officials.
William A. Dombi, President of the National Association for Home Care and Hospice (NAHC), opposed the proposed 8.01% behavioral reduction in payment rates, arguing in Home Health Care News that CMS should not base adjustments on assumed behavior changes in response to PDGM’s implementation but rather on actual behavioral changes. The final 4.36% reduction in payment rates, although less painful, is still based on assumed changes in home health agency behaviors during the transition to PDGM as CMS works to calculate the payment rate in a budget-neutral manner for 2020.
Many home health officials are worried that PDGM will not be budget neutral, however, and that the new reimbursement strategy could lead to shaky financial standing. Are you worried too?
Hitting Close to Home
To understand the implications for your specific agency, you will need to do some advance research and planning, and arrange for training before the January 1 PDGM start date.
Making an educated prediction about the future revenue impact of PDGM for your organization requires a look back at your past claims with CMS. In a Relias-BlackTree Healthcare Consulting webinar on critical steps to take in planning for PDGM, BlackTree Managing Principal Todd Montigney advises using CMS resources to help.
Montigney notes that officials can download PDGM files from the CMS Home Health Agency (HHA) Center web page. These files include detailed information and projections for 2020, such as calculations showing agency-level impacts of PDGM, case-mix weights, and LUPA thresholds.
You can also get a clearer picture by analyzing your past billing data to see trends in the following aspects:
- Most common diagnosis codes.
- Average number of visits per patient.
- Average number of periods per patient.
- Trends in LUPAs incurred.
To put your agency in the best position to transition to PDGM, you will also need to analyze performance in these areas:
- Turnaround time for completing the patient assessment and the Outcome and Assessment Information Set-D1 (OASIS-D1).
- Time between start of care and CMS-485 form being sent to physician.
- Standard procedure for following up with physicians to ensure orders are signed.
- Average turnaround time for physicians to sign form CMS-485.
Choosing Diagnosis Codes Wisely
Montigney notes that completing the OASIS-D1 promptly and including all relevant diagnosis codes are essential steps. PDGM breaks down to 432 different case-mix groups with HIPPS codes, and each HIPPS code has a visit threshold for LUPAs. Case managers need that information to effectively manage patient visits to reduce LUPAs.
CMS provides an overview of how the groupings are determined in the figure below.
Figure: Structure of the Patient-Driven Groupings Model
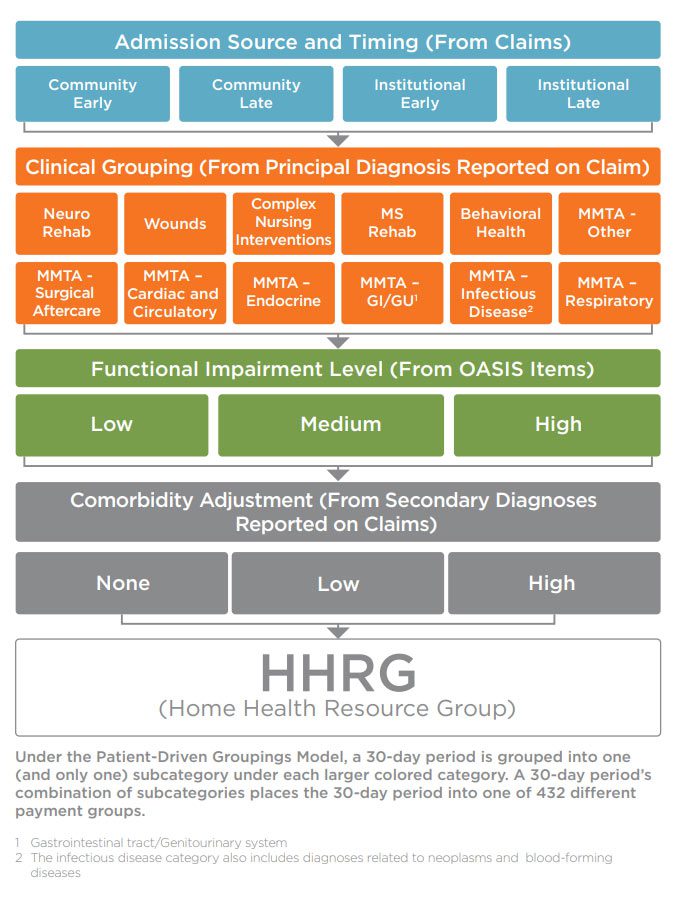
Supervisors will need to be sure intake and coding staff are aware of the primary and secondary diagnosis codes acceptable under PDGM and that the claims actually reflect those required codes. Up to 25 diagnosis fields are available for claims, and the combined secondary diagnoses will be used to determine the comorbidity adjustment.
Some diagnosis codes would be considered questionable encounters if submitted as the primary diagnosis. These represent an aspect of the patient’s condition but do not constitute home health eligibility on their own, as BlackTree Consulting Director Brian Harris says in a follow-up to his Relias-BlackTree webinar on PDGM billing and finance.
Maintaining Quality Care and Financial Strength
Amid so many changes related to transitioning to the new payment model, the quality of care given to patients should not change. However, the type of care an agency chooses to provide and the complexity of the patients it chooses to serve just might.
When the new payment model becomes reality, Harris notes, agencies will have the challenge of evaluating their case mix to determine if it is sustainable under PDGM. If not, more change will be necessary.

Toolkit: Preparing for PDGM
Discover 4 key facets to consider as you create your plan for PDGM. Prepare your organization with 5+ free resources, including white paper, webinars, guides and more.
Get the toolkit →